
Japet research center in partnership with the ergonomics division of a major French energy group.
1. Introduction
Lower back problems are becoming increasingly common in industrialized countries. It is estimated that 80% of the current adult population has or will suffer from low back pain, with an annual prevalence of 30% (Olivier N., 2016). This frequency more than tripled in France between 1980 and 2000. Epidemiological studies are very numerous and confirm a similar prevalence in the various industrialized countries. Chronic low back pain, by definition greater than three months, concerns 20% of low back pain, which represents between 10% and 20% of the population, with the preferred age being between 35 and 45 years old.
Low back pain is a major public health problem and a burden on the economy because it generates significant costs that can reach 20 billion euros per year in France (Thevenon A., 2015) (Dogan C., 2016). Low back pain is one of the most expensive illnesses for businesses. It is responsible for 10% of work stoppages, all sectors combined, and for 13% of disability claims.
Ergonomists have a very important role because they study the risks associated with the workplace in order to adapt them to operators. When adapting the workstation is not possible, ergonomists sometimes turn to other solutions such as robotization or the installation of exoskeletons. However, it is necessary to assess the impact of a new solution, before, during and after its implementation. In the literature, exoskeletons used in the workplace are assistive and preventive devices aimed at reducing the loads on the body and in the various joints. The device we are proposing to study is a medical exoskeleton that aims to prevent and relieve pain in order to keep workers employed. This case study is a first evaluation of the implementation of a lumbar exoskeleton on a painful back activity in the workplace: The port of heavy loads.
2. Materials and methods
2.1. Approach
This case study is carried out on an agent of a French energy company. The impact of manipulation on the spine varies according to The type of object to transport, The height and The distance charges, The type of plug and The repetition frequency movements. The case study presented is part of a workplace study conducted by an ergonomist and occupational psychologist from the energy company.
2.2. Subject
This exoskeleton is intended for a population suffering from lower back pain, and especially pain related to mechanical pathologies. Only one subject was recruited for this case study. The subject provided informed consent. The volunteer is suffering from low back pain column.
2.3. Equipment and instrumentation
2.3.1. Lumbar exoskeleton
The worn exoskeleton is a dynamic trunk orthosis that applies vertical traction forces to reduce pressure on the lumbar spine (Japet Medical, France). The device consists of two belts, one on the hips and the other on the lower ribs. These two belts are connected by two sets of actuators positioned on either side of the body.
The four actuators have a double role: preserve the mobility of the trunk while applying traction force. Each actuator is connected to the belts by a ball joint and automatically adapts to different heights, allowing the movement of the trunk to be followed (Fig. 1). The exoskeleton has four levels of traction force, 4 kg, 8 kg, 12 kg, and 16 kg.

2.3.2. Motion capture system
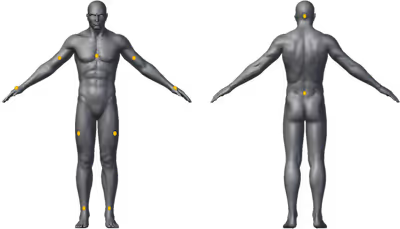
The acquisition of posture is achieved thanks to Eleven inertial measurement units (TEA Captiv T-Sens Motion, TEA), placed on the hands, arms, arms, head, head, sternum, trunk (lumbar part), thighs and shins (Fig. 2). Data acquisition is carried out at 64 Hz. Wireless communication between the sensors and the data logger (TEA Captiv T-LOG, TEA) allows the subject to be free to move in a natural and realistic manner. The data is immediately transmitted to the computer, which Allows you to visualize the movements of the subject via the Captiv software (TEA). This software performs an ergonomic evaluation for each record in .pdf format. However, to facilitate processing, the data is retrieved in .csv format to be analyzed on Matlab (MathWorks®).
2.4. Experimental procedure
A first study on the workstation of a handling operator was carried out by the ergonomist. This workstation cannot be adjusted to ergonomic standards, which is why the ergonomist proposed to test a lumbar exoskeleton in order to relieve his back during his professional activities.
After validating the device's indications with the manufacturer, the ergonomist presented the exoskeleton and the course of the study to the volunteer. The operator gave informed consent. Anthropometric measurements are collected, including weight, height, height, hip circumference, and underchest circumference, by the ergonomist. These measurements make it possible to predict the correct size of the device for the test.
On the day of the test, a member of the Japet team and the ergonomist went to the storage shed where the subject works. The subject is informed about the operation of the device and the measurements taken during the test. Then, the subject tried the exoskeleton to become familiar with the product and its control interface. After that, the exoskeleton was removed in order to place the inertial measurement units (IMUs). Finally, the exoskeleton is put back in place to check that it is not pressing on the IMU.
The test includes three different tasks: unloading boxes (two pallets are placed on the ground, the subject transfers the cardboard from one pallet to the other), Storing tires on shelves (the subject must lift a tire from the ground up to a 1.5 m high shelf) and Moving a gas bottle (the subject must lift a gas bottle off the ground and put it back on the ground 5 m away). The subject is responsible for carrying out the tasks in the most natural way possible. The same tasks are repeated without the device and with the device (traction force of 2 kg/actuators).
Six recordings are made (Fig. 3). For each of them, the IMU is calibrated using the Captiv software. To perform the calibration, the subject must maintain an orthostatic position with his arms extended for 10s.

3. Results
Each segment defined by the IMU is assumed to be a rigid, non-deformable solid. Connections between segments are assumed to be perfect with no translational degrees of freedom (DOF). The IMU then makes it possible to evaluate the angles formed by the joints of the neck (3 DOF), back (3 DOF), shoulders (3 DOF), elbows (2 DOF), wrists (2 DOF), wrists (2 DOF), hips (3 DOF), hips (3 DOF), and knees (2 DOF). In this study, we are only interested in At the three angles of the back.
3.1. Unloading cartons
When unloading boxes, the acquisition lasted throughout the activity (78s), that is to say that several boxes have been moved.The 2D graphs (Fig. 4) represent the data without the device (blue) and the data with the device (cyan).

Data without the device is more scattered than data with the device.
The abscissa and ordinate axes have three colors, referring to the three angular areas of the back (Table 1.) commonly used by ergonomists. CAPTIV references: the comfort zone (green), the risk zone (orange), and the danger zone (red).
Comfort areaRisk areaDangerous areaFlexion extension] -10°; 35° [[-20°; -10°] and [35°; 45°] -20° and > 45°Lateral inclination] -10°; 10°; 10° [[-20°; -10°]; 10° [-20°; -10°] and [10°; 20°] -20° and > 20°Axial rotation] -15°; 15° [[-30°; -10°; -10°] and [10°; 20°] -20° and > 20°Axial rotation] -15°; 15° [[-30°; -10°; -10°] 15°] and [15°; 30°] -30° and > 30°
Table 1. Angular areas of the back
By comparing the acquisition data with the angular areas table From the back (table 1), it is possible to quantify the percentage of time spent in each zone. To do this, it is necessary to make an assumption about the combinations of angles, which are not taken into account in this table. We made the decision not to consider combinations of movements, but to look at the three angles independently (flexion-extension, lateral inclination, and axial rotation).
Below is the percentage of time spent in each zone when unloading boxes:
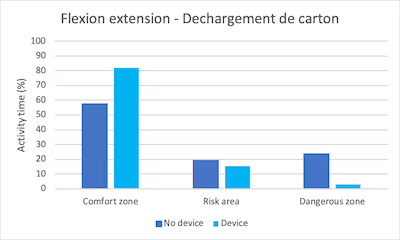
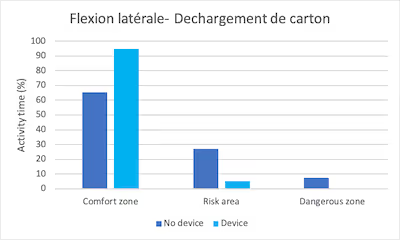

Fig. 5. Percentage of time spent in the various angular areas while unloading cartons
The subject spent more time in the comfort zone with the device than without flexure, extension, lateral, and axial rotation. He spent less time in risk areas as well as in dangerous areas thanks to the device.
3.2. Storing tires on shelves
In order not to disrupt the operator's activity, the acquisition was carried out on the storage of only two tires (16s).
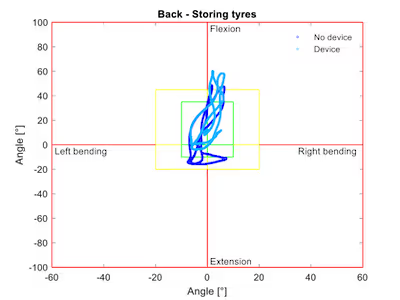
Fig. 6. Scatter plot representing back angles (angles of flexion/extension as a function of lateral inclination) during tire storage.
The figure (Fig. 6) does not show a significant difference in dispersion between the curves without and with the device. The percentage of time spent in each comfort zone for the storage tire is as follows:
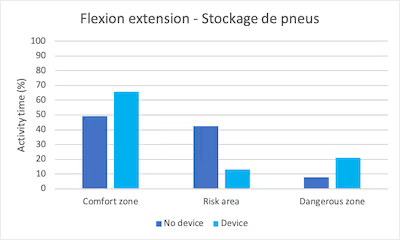
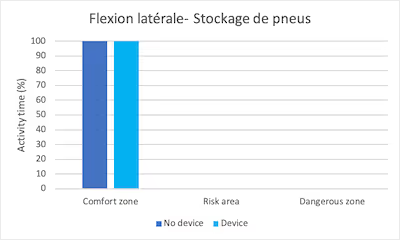
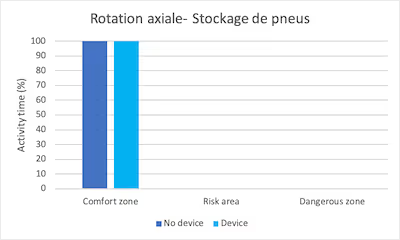
Fig. 7. Percentage of time spent in the various angular areas during the tire storage task
The subject spent more time in the flexure extension comfort zone with the device than without (65.8% of the time and 49.4% of the time respectively). The time spent in the risk zone is reduced with the device (13.3% with the device and 42.6% without). The time spent in the danger zone increases with the device (20.9% with the device and 8% without).
Finally, with or without the device, the subject spends 100% of the time in the comfort zone in lateral inclination and in the comfort zone in axial rotation.
3.3. Moving a gas bottle
For the same reasons as the tire storage test, the acquisition was carried out for the movement ofa single gas bottle (13s).
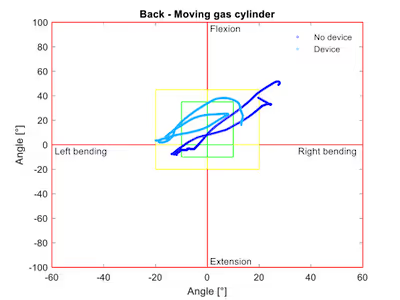
Fig. 8. Scatter diagram representing back angles (angles of flexure and extension as a function of lateral inclination) during the movement of gas cylinders.
The data with the device seems to be less scattered than the data without the device. The percentage of time spent in each comfort zone for the gas bottle in motion is as follows:
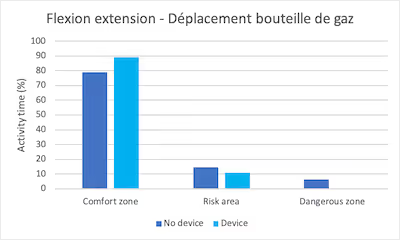
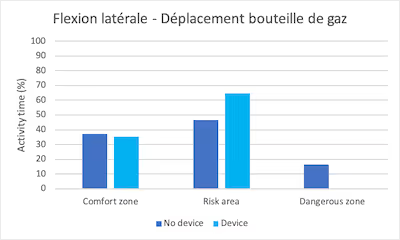
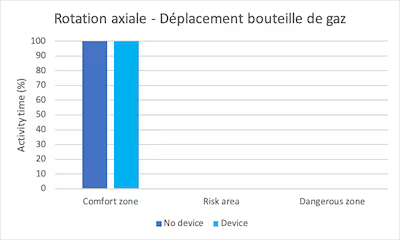
Fig. 9. Percentage of time spent in the various angular areas during the gas cylinder task in motion
In flexure extension, the subject spent 78.9% of the time in the comfort zone, 14.6% in the risk zone, and 6.5% in the danger zone without the device. With the device, he spent 89% of the time in the flexure extension comfort zone and 11% in the risk zone.
The subject spent 37.1% of the time in the comfort zone on a lateral incline without the device, 46.5% in the risk zone and 16.4% in the danger zone. With the device, he spent 35.2% of the time in the comfort zone and 64.8% in the risk zone.
Finally, with or without the device, the subject spent 100% of the time in the comfort zone in axial rotation.
4. Discussion
The device seems to have a generally positive impact on the postures taken by the operator. In fact, two of the nine graphs stand out: the flexion-extension movement during the task of storing the tires, and the lateral inclination during the task of moving the gas cylinder.
During the tire storage task, the flexure extension results are questionable. Indeed, the time spent in the comfort zone is more important with the device than without it, but the danger zone is more important with the device than without it. Summarizing the time spent in the risk zone and the dangerous zone, it appears that the operator spent 50.6% of the time in a bad posture without the device, and 34.2% of the time in a bad posture with the device. Note that the device is not designed to work with your arms in the air. This may explain these poor results for storing tires on a high shelf.
With regard to the results of the lateral inclination while moving the gas bottle, the operator spent almost as much time in the comfort zone without and with the device (37.1% and 35.2% respectively). The percentage of time spent in the risk zone with the device is significantly higher than without the device, but wearing the device allows the operator not to take a position in the danger zone. Summarizing the time spent in the risk zone and the dangerous zone, it appears that the operator spent 62.9% of the time in a bad posture without the device, and 64.8% of the time in a bad posture with the device.
So the result of this case study is very encouraging.
However, this preliminary work has numerous limitations. First of all, it is a case study on a single operator. This study should be extended to a larger scale. Second, there was little repetition of tasks. Indeed, it is difficult to carry out measurements in a real work situation because the implementation of the protocol necessarily slows down the operator's work pace. Thirdly, it would be interesting to conduct a whole-body study in order to analyze the impact of the device on other joints in the body.
5. Conclusion
This preliminary case study showed that the device has a positive impact on the posture adopted by the operator in 88.9% of use cases. A broader assessment is needed to confirm these encouraging data.
6. Thanks
We thank the volunteer operator and his manager for the time they devoted to us for this study.
7. References
Dogan C., D.A. (2016). Gender as a modifying factor influencing myotonic dystrophy type 1 phenotype severity and mortality: A nationwide multiple databases cross-sectional observational study. PLoS One, 11 (2) :e0148264.
Olivier N., B.J. (2016). Evaluation of muscle oxygenation by near infrared spectroscopy in patients with facioscapulohumeral muscular dystrophy. NeuroMusculdisORD NMD, 26 (1) :47-55.
Thevenon A., G.F. (2015). Collection of normative data for spatial and temporal gait parameters in a sample of French children aged between 6 and 12. Ann. PhysRehabil Med., 58 (3) :139-44.



